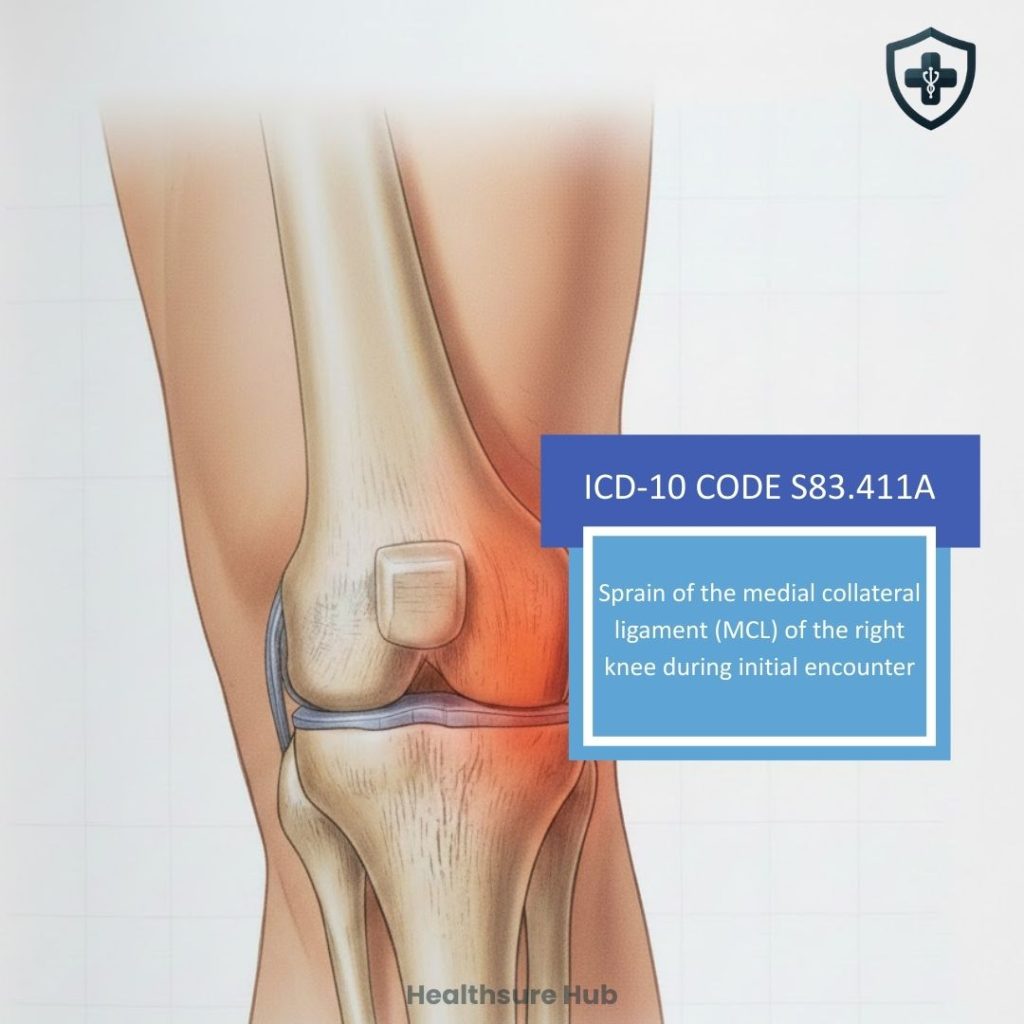
Knee injuries are common, particularly among athletes, active adults, and older adults. Yet, when it comes to medical coding, even a seemingly simple knee sprain requires precision. One specific ICD-10 code for knee injuries is S83.411A, which represents a sprain of the medial collateral ligament (MCL) of the right knee during the initial encounter.
Whether you are a medical coder, a clinician, or a curious patient, understanding S83.411A can prevent errors and improve patient outcomes. Our team at HealthSure Hub, delves into its clinical and coding relevance, documentation requirements, common mistakes, and related guidelines.
Overview of ICD-10 Code S83.411A
S83.411A falls under the “S” chapter of ICD-10, which covers injuries to specific body regions. This code is used when the right knee’s MCL is sprained, and the patient is receiving active treatment for the first time.
The “A” extension indicates an initial encounter—the patient’s first visit where the injury is being treated.
When the Initial Encounter Extension Applies
The “A” extension is used whenever the patient is in the active treatment phase for the right knee MCL sprain:
- First visit to an emergency department or urgent care following trauma
- Initial orthopedic evaluation
- Imaging referrals where MCL injury is suspected or confirmed
Later visits, rehabilitation follow-ups, or long-term complications would use subsequent encounter (D) or sequela (S) codes.
Breaking Down the Code
Every ICD-10 code conveys specific information. Here’s a clear breakdown:
| Code Segment | Meaning | Explanation |
| S83 | Injury of knee and lower leg | Refers to the general body region affected. |
| .411 | Sprain of medial collateral ligament, right knee | Specifies the ligament involved and laterality. |
| A | Initial encounter | Indicates first active treatment visit. |
Related codes for reference:
- S83.412A – MCL sprain, left knee, initial encounter
- S83.419A – MCL sprain, unspecified knee, initial encounter
- S83.511A – ACL sprain, right knee, initial encounter
This hierarchy ensures consistent medical documentation, accurate insurance claims, and reliable national injury statistics.
Specificity matters. Using the wrong code can lead to claim denials, misrepresentation of patient records, and confusion in treatment planning.
What a “Medial Collateral Ligament Sprain” Means
While S83.411A is primarily a coding designation, it also reflects the clinical condition:
- The MCL stabilizes the inner knee, preventing inward bending.
- A sprain occurs when the ligament is stretched or partially torn, often from twisting, sudden direction changes, or direct impact.
- Patients may experience knee pain, swelling, tenderness, or limited mobility on the inner side of the right knee.
Even if the exact grade of the sprain (mild, moderate, or severe) is not specified in documentation, the code applies as long as it is the initial encounter for active treatment.
S83.411A by the Numbers
Medial collateral ligament (MCL) injuries are among the most frequently documented knee ligament injuries in both sports medicine and general orthopedic care.
- MCL injuries account for an estimated 40% of all knee injuries, making them one of the most common ligament sprains of the knee.
- MCL injuries often occur due to some sports-related trauma, particularly in soccer, football, and skiing. In skiing, particularly, 60% of skiing knee injuries involve the MCL.
- Grade I and II MCL sprains are most common and are typically managed non-surgically, often resulting in shorter recovery timelines but frequent follow-up encounters requiring accurate encounter sequencing.
- Claims submitted with incomplete injury documentation are more likely to experience payment delays or requests for additional medical records, increasing administrative burden for providers.
These trends highlight why precise use of S83.411A during the initial encounter is essential not only for clinical clarity but also for clean claim submission and reimbursement.
Common Claim Denials and Payer Red Flags
Although S83.411A is a straightforward injury code, claims associated with knee sprains are frequently reviewed by payers due to high utilization and variability in documentation.
Common denial triggers include:
- Missing or unclear laterality – Documentation that references “knee sprain” without clearly specifying the right knee can result in denials or downcoding.
- Incorrect encounter sequencing – Using the initial encounter code (A) for follow-up visits, rehabilitation sessions, or ongoing care may trigger payer audits or claim rejections.
- Lack of medical necessity support – Imaging, bracing, or physical therapy services billed alongside this code may be denied if clinical notes do not adequately support the need for those services.
- Diagnosis–procedure mismatch – Payers may flag claims when the diagnosis code does not logically align with reported CPT procedures, especially in orthopedic and rehabilitation billing.
- Overuse of unspecified injury codes – Failure to use a specific code like this one when documentation supports it can raise compliance concerns and affect reimbursement accuracy.
Addressing these documentation and coding issues at the initial encounter helps reduce rework, avoid denials, and ensure consistent reimbursement across the full episode of care.
Clinical Scenarios Where S83.411A Is Used
This ICD-10 is often applied in real-world clinical settings, such as:
- A soccer player twisting the knee during a pivot
- An adult slipping on ice and experiencing inner knee pain
- First-time orthopedic evaluations where the MCL sprain is confirmed through examination or imaging
In these situations, the focus is on documenting the injury, laterality, and treatment, rather than grading the exact severity unless specified.
Common Documentation Gaps
This code is sometimes selected due to real-world clinical documentation patterns:
- Initial evaluation may focus on stabilization rather than detailing ligament grade
- Clinicians may simply record “right knee pain” or “MCL sprain” without additional specifics
- Imaging may confirm injury but not specify associated tissues
These practices reflect workflow realities rather than errors in care.
When to Use
S83.411A is used only during the initial encounter for active treatment of a right knee MCL sprain. Examples include:
- Emergency room or urgent care visits following a sports injury or fall
- Outpatient orthopedic consultations for acute MCL injuries
- Physical therapy evaluation immediately following the injury
It should not be used for:
- Follow-up visits (subsequent encounter codes apply)
- Sequela, or long-term complications (sequela codes apply)
- Left knee or unspecified MCL injuries
Accurate timing ensures that treatment is properly captured and reimbursed.
Clinical Documentation Requirements
Proper documentation is critical for accurate coding. Clinicians should record:
- Laterality – Right knee
- Type of injury – Sprain of the MCL
- Encounter type – Initial (active treatment)
- Severity or grade – Optional but helpful (Grade I–III)
- Associated injuries – Note if present, as they may require additional codes
Without clear documentation, coders may have to use unspecified or incorrect codes, which can result in compliance issues and delayed reimbursement.
Clinical Relevance of Accurate Coding
Proper coding of this ICD-10 code has significant implications beyond billing:
- Patient care: Accurate codes ensure continuity of care, correct referrals, and appropriate treatment plans.
- Insurance and reimbursement: Prevents claim denials and ensures correct payments.
- Research and population health: Supports reliable injury statistics, trend analysis, and resource allocation.
An MCL sprain may appear minor, but its precise coding contributes to larger clinical and administrative systems.
Conclusion
S83.411A is more than a code, it is a critical component of clinical documentation, billing accuracy, and patient care continuity. By understanding when and how to use this code, coders and clinicians can prevent errors, ensure proper reimbursement, and support research and population health initiatives. For patients, accurate coding translates to clear medical records, appropriate treatment, and reduced risk of administrative issues.
Meticulous attention to laterality, encounter type, and injury specifics makes all the difference. Whether you are coding, treating, or studying knee injuries, S83.411A ensures clarity and precision in healthcare documentation.