Falls are one of the most common yet often under-documented injuries in healthcare. When a patient presents after a fall, but the exact circumstances are unclear, how do coders and clinicians accurately capture the event? At HealthSure Hub, we specialize in helping healthcare organizations navigate coding and documentation challenges, including the correct use of ICD-10-CM code W19.XXXA.
What Is ICD-10 Code W19.XXXA?
W19.XXXA is a medical ICD-10-CM code that is used to classify unspecified fall, initial encounter. It captures the cause of injury without detailing the exact mechanism, location, or circumstances of the fall.
In practice, this specific ICD-10 code is applied when a patient presents for the first time after a fall, but the medical record does not specify how the fall occurred. The code helps medical coders indicate the external cause of injury, which is critical for insurance claims, public health reporting, and injury surveillance. It does not describe the injury itself, that is captured by a separate diagnosis code such as a fracture, contusion, or sprain.
Breakdown of the ICD-10 Code Structure
| Character | Meaning |
| W | External causes of morbidity |
| 19 | Unspecified fall |
| XXX | Placeholder characters indicating no additional specificity |
| A | Initial encounter (active treatment) |
The placeholders (X) are required to maintain the 7-character structure of ICD-10-CM codes. The 7th character “A” specifies that the patient is receiving active treatment for the injury resulting from the fall.
83% of hip fracture deaths and 88% of emergency department visits and hospitalizations for hip fractures were caused by falls.
Understanding the Purpose of External Cause Codes
ICD-10-CM external cause codes, found in Chapter 20 (V00–Y99), describe how an injury or adverse event occurred. The code differs from diagnosis codes because it does not identify the injury, illness, or condition. Instead, it complements the injury code to provide context for:
- Patient care documentation
- Medical billing and reimbursement
- Epidemiological tracking of injuries
- Public safety and prevention programs
Falls are also the leading cause of traumatic brain injuries (TBIs), highlighting the critical need for accurate coding and injury tracking.
Accurately applying external cause codes ensures compliance with coding guidelines and helps healthcare organizations generate meaningful data on injury patterns.
When Is W19.XXXA Appropriate to Use?
This ICD-10 code should be used in situations where:
- The medical record does not specify the fall’s mechanism, environment, or surface.
- The patient is seen for the first time following the fall.
- Documentation does not allow the use of a more specific fall code, such as slipping, tripping, or falling from a height.
Typical clinical settings include:
- Emergency department visits
- Urgent care evaluations
- Initial inpatient or outpatient assessments
It is crucial for coders to review documentation carefully. If additional details are available, a more specific fall code should be used instead.
Initial Encounter Explained
The 7th character “A” in W19.XXXA indicates an initial encounter, meaning the patient is receiving active treatment for injuries related to the fall. This includes interventions such as:
- Surgical procedures
- Emergency care
- Diagnostic evaluation and management
- Casting or splinting
This distinguishes the initial encounter from:
- Subsequent encounters (D): Follow-up visits for continued care or healing
- Sequela (S): Late effects or complications arising from the original injury
Correctly identifying the encounter type ensures proper claim processing and compliance with ICD-10-CM guidelines
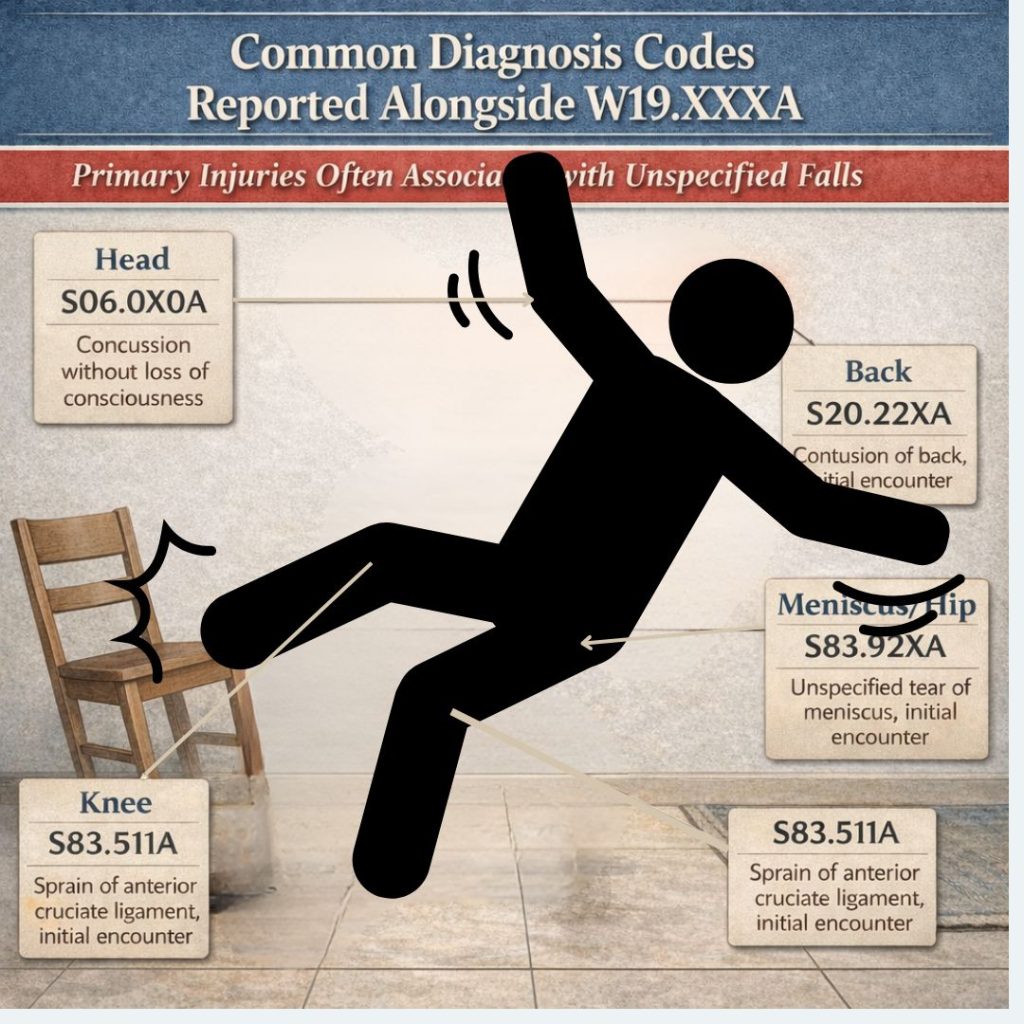
Common Diagnosis Codes Reported Alongside
External cause codes like W19.XXXA are almost always used in conjunction with a primary injury code. Examples include:
- Fractures: S83.92XA (Unspecified tear of meniscus, initial encounter)
- Contusions: S20.22XA (Contusion of back, initial encounter)
- Sprains and strains: S83.511A (Sprain of anterior cruciate ligament, initial encounter)
- Head injuries: S06.0X0A (Concussion without loss of consciousness)
In claims, the primary injury diagnosis should be listed first, followed by the external cause code. This sequencing improves clarity and ensures proper reimbursement.
Coding Guidelines and Documentation Best Practices
ICD-10-CM official guidelines recommend using external cause codes:
- Whenever the cause of injury is known or suspected
- In all initial encounters for injury-related care
- To support injury surveillance and reporting initiatives
Best practices include:
- Confirming that the patient’s record supports the use of an unspecified fall
- Adding W19.XXXA after the primary diagnosis code
- Avoiding use if more specific fall codes are documented
Adhering to these guidelines reduces coding errors and supports compliance in audits and review.
Common Coding Errors
Frequent mistakes with the code include:
- Using the code when the fall details are documented (specific code should be used instead)
- Omitting the 7th character, which can result in claim denial
- Applying the code to subsequent encounters
- Using it as a primary diagnosis rather than an external cause
Avoiding these errors requires careful review of documentation and understanding of ICD-10-CM conventions.
Conclusion
W19.XXXA should be used to document an unspecified fall during the initial encounter and always paired with the primary injury code. As an external cause code, it ensures accurate reporting, proper claims processing, and compliance with ICD-10-CM guidelines.
At HealthSure Hub, we emphasize precise coding practices to ensure every fall is properly recorded, claims are processed correctly, and healthcare organizations can rely on accurate data for both patient care and reporting.