Your hands are essential tools for nearly every aspect of daily life, from typing on a keyboard to cooking a meal or performing precise manual tasks. Yet, minor injuries such as cuts or open wounds can happen in the blink of an eye. These seemingly small injuries, if not properly documented and treated, can lead to infection, reduced function, or complications that affect quality of life. One code commonly used for hand injuries is ICD-10 S61.209A which represents an unspecified open wound of an unspecified finger without damage to the nail, during the initial encounter.
Our team at Healthsure Hub breaks down the code and explains why proper coding ensures these injuries are captured correctly in medical records, facilitating optimal care and reimbursement.
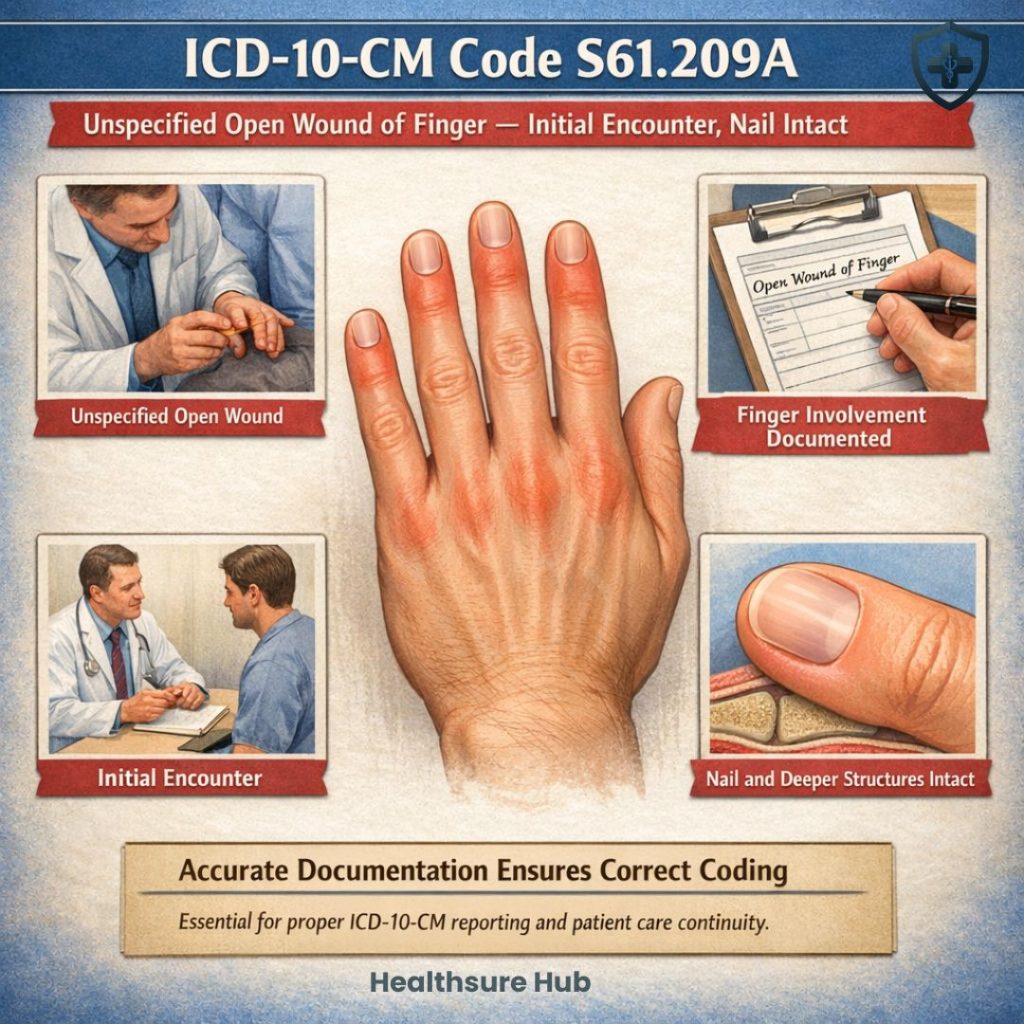
What is ICD-10-CM Code S61.209A?
From a billing perspective, S61.209A is applied when a patient presents with a finger laceration or cut, but the documentation does not specify which finger or the exact nature of the wound.
This situation often occurs in urgent care or emergency settings where immediate treatment takes priority over detailed anatomical description.
Using this code allows healthcare providers to record the condition, justify treatment such as wound cleansing or suturing, and submit insurance claims that reflect the services performed. It also preserves continuity in the patient’s medical history so future providers understand the nature of the original injury.
The final letter “A” is not arbitrary, it indicates that the visit is an initial encounter, meaning the patient is receiving active treatment for the injury. If the patient returns for follow-up care, a different encounter character would be required.
Choosing the Right Code Requires Careful Review of Documentation
Although S61.209A is valid, it is considered an unspecified code. Medical coders are expected to select the most detailed diagnosis available in the documentation. If the provider notes nail damage or identifies the exact finger, a more specific code should be used instead. For instance, there are separate classifications for wounds involving nail injury or for wounds affecting other parts of the hand.
Because insurers sometimes scrutinize unspecified codes, detailed charting benefits both clinical accuracy and reimbursement efficiency. Clear notes about wound depth, location, and associated findings can prevent claim delays and reduce requests for additional information.
Coding Guidelines and Related Codes
The “A” in S61.209A specifies an initial encounter, meaning the first medical visit for this injury. Related ICD-10-CM codes include:
- S61.9XXA – Open wound of unspecified finger with nail damage
- S61.8XXA – Open wound of other specified parts of the hand
Coders should select the most precise code based on documentation; “unspecified” is only appropriate when finger location or wound type is unknown.
Common Causes of Unspecified Finger Wounds
Finger injuries can occur in a variety of settings:
- Accidental cuts from kitchen knives, glass, or office tools
- Work-related trauma in industrial, mechanical, or office environments
- Sports-related incidents, including ball handling or falls
Most of these injuries are minor and do not involve nail damage or deeper structures like tendons or bones, which makes S61.209A the correct code for initial treatment. In the U.S., approximately 2.8 million emergency department visits occur each year due to hand and finger injuries.
Besides the common causes of finger wounds, many of these injuries are linked to falls or accidents, and could be listed with related ICD-10 codes such as ICD-10 for falls either without knowing how the fall occurred or on the same level.
A Real-Life Example
Imagine a graphic designer rushing to prepare dinner after work. While chopping vegetables, the knife slips and causes a small but deep cut on one finger. The bleeding doesn’t stop after several minutes, so she visits an urgent care clinic.
The clinician cleans the wound, confirms there is no nail damage or tendon involvement, and closes it with a few sutures. Because the chart does not specify which finger was injured and the wound description is limited, the coder assigns S61.209A. The code accurately reflects what is known at the time and allows the visit to be billed correctly while still documenting the injury for her medical record.
Symptoms and Clinical Presentation
Patients with an unspecified finger wound may present with:
- Bleeding, redness, or swelling around the wound
- Pain localized to the affected finger
- Limited mobility or tenderness
- Visible open wound without nail damage
Immediate evaluation is essential to rule out more severe injury and prevent infection.
Medical Documentation Requirements
AccAccurate coding always begins with accurate documentation. Providers should note that the injury is an open wound, confirm whether the nail or deeper tissues are involved, and indicate that the encounter is the first visit for treatment. These details ensure that the selected diagnosis code truly matches the clinical picture.
Complete records do more than support billing. They also create reliable data that can be used to track injury trends, guide workplace safety initiatives, and inform public health research. Inconsistent or vague documentation, on the other hand, can lead to claim denials, audits, or gaps in patient history.
Treatment and Management
Management typically starts with immediate first aid, cleaning the wound, applying antiseptic, and covering it with a sterile dressing. Medical professionals may then examine the injury more closely to check for foreign bodies or structural damage. Larger or deeper cuts sometimes require sutures or adhesive closure.
Follow-up visits are often recommended to monitor healing and watch for signs of infection. These subsequent appointments are not coded with S61.209A, since that designation applies only to the initial treatment encounter.
Importance of Proper Coding for Healthcare Providers
Accurate coding is crucial for multiple reasons:
- Ensures correct insurance reimbursement for services rendered
- Maintains reliable health records, supporting clinical decisions
- Enables tracking of injury patterns and epidemiological data for public health purposes
- Reduces the risk of billing errors, audits, or claim denials
Correct application of S61.209A not only impacts the provider financially but also supports high-quality patient care.
Conclusion
ICD-10 S61.209A plays a crucial role in accurately documenting and billing, particularly when the exact finger or wound details are not fully specified, ensuring that healthcare providers can still record and treat the injury appropriately.
Proper use of the code supports accurate insurance claims, thorough medical records, and effective patient care tracking. Given the millions of finger injuries that occur annually, applying this code correctly is essential for both clinical and administrative accuracy.