Cancer does not always end when treatment stops. Even after a malignancy has been successfully treated, its presence in a patient’s medical history continues to shape clinical decisions, preventive care strategies, and insurance coverage. As cancer survivorship continues to rise globally, accurately documenting a patient’s cancer history has become more important than ever.
This is where ICD-10-CM code Z85.9 plays a critical role. At Healthsure Hub, we help healthcare professionals understand how codes like this one ensure accurate documentation, compliant billing, and better long-term care for patients with a history of cancer.
What Is ICD-10-CM Code Z85.9?
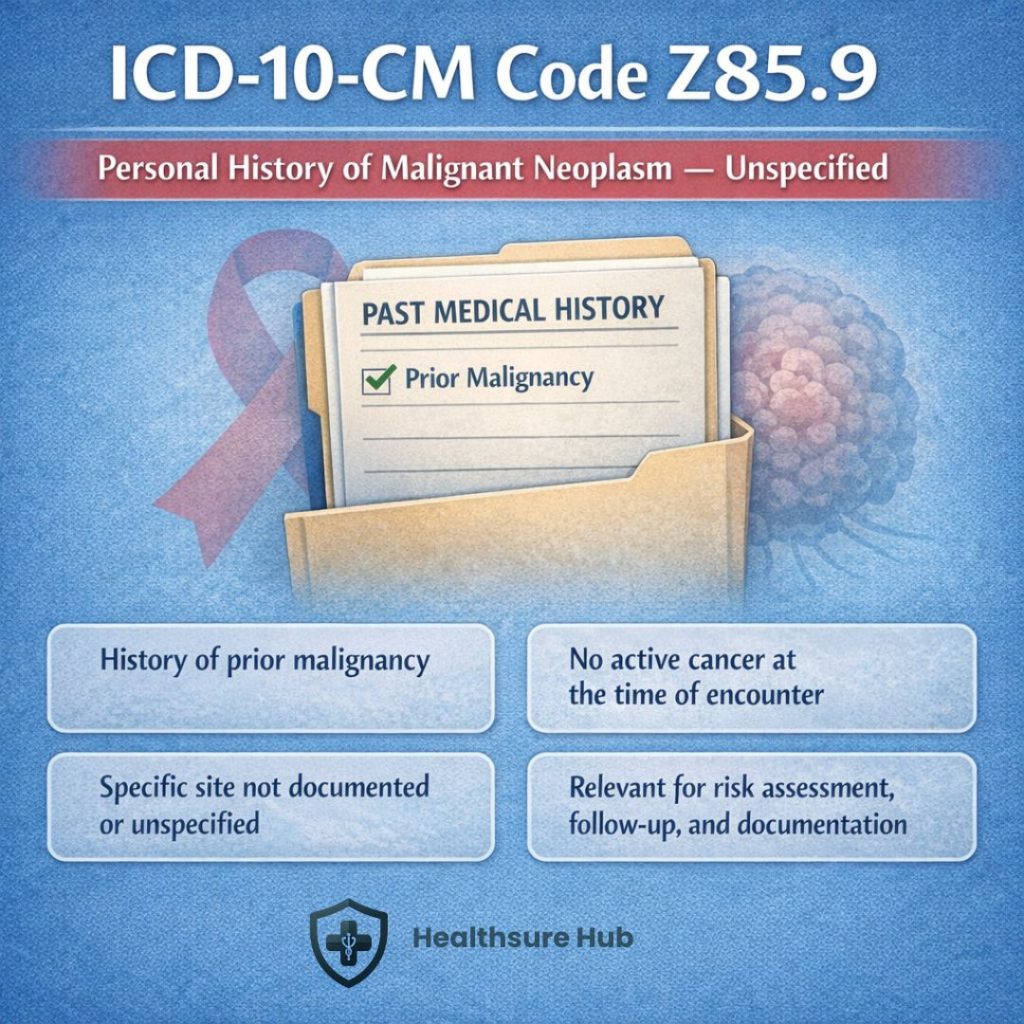
ICD-10-CM code Z85.9 is defined as personal history of malignant neoplasm, unspecified. It is used to indicate that a patient has had a prior diagnosis of cancer, but the malignancy is no longer active, and the specific site of the cancer is not documented or not specified.
From a medical billing perspective, this ICD-10 code communicates that:
- The patient does not currently have cancer
- The history of cancer remains clinically relevant
- The condition may influence screening, monitoring, or treatment decisions
This code belongs to Chapter 21 of ICD-10-CM, which includes factors influencing health status and encounters with health services. It is frequently reported during preventive visits, chronic care management, preoperative evaluations, and specialty follow-ups.
Why Z85.9 Matters in Clinical Documentation and Coding
A documented history of malignant neoplasm affects far more than oncology visits. Patients with a prior cancer diagnosis often require:
- More frequent screenings
- Ongoing surveillance
- Modified treatment plans
- Closer monitoring for recurrence or secondary malignancies
According to data from the National Cancer Institute, the number of cancer survivors continues to grow each year, with tens of millions of individuals living with a history of cancer worldwide. Improved detection and treatment have significantly increased survival rates, making accurate survivorship documentation essential for modern healthcare systems. Z85.9 ensures this history is not lost when active treatment ends.
When to Use Z85.9 vs. Other Personal History of Cancer Codes
This specific ICD-10 code should only be used when the specific site of the prior malignancy is unknown or unspecified. ICD-10-CM includes numerous site-specific personal history codes (Z85.0–Z85.89), which should be used whenever documentation supports greater detail.
Payers and auditors generally prefer site-specific history codes when available, as they provide clearer clinical context. This code is appropriate when:
- Historical records lack specificity
- The provider documents “history of cancer” without naming the site
- The cancer site cannot be determined
Globally, the World Health Organization (WHO) reports that survival rates have improved significantly due to early detection and advances in treatment, with 5-year survival rates exceeding 70% for many common cancers in high-income countries. Using Z85.9 when more specific information exists may increase audit risk.
Documentation Requirements for Accurate Use
Clear documentation is essential for proper use of this code. The medical record should indicate:
- A confirmed history of malignant neoplasm
- That the cancer is no longer active
- That the site is unspecified or unknown
Acceptable provider language may include:
- “History of cancer”
- “Personal history of malignant neoplasm”
- “Status post cancer treatment”
Vague or incomplete documentation can lead to miscoding, delayed claims, or compliance issues.
Common Coding Errors and Compliance Risks
Errors involving this code often stem from confusion between history and active disease. Common mistakes include:
- Using this code when the patient has current or active cancer
- Reporting this code instead of a site-specific history code
- Confusing this code with Z08 (follow-up examination after cancer treatment)
Misuse can result in claim denials, inaccurate risk profiles, or audit exposure. A personal history of cancer, coded with Z85.9, is critical for risk stratification, as survivors face a higher risk of developing secondary malignancies.
Z85.9 and Preventive Care, Screening, and Risk Stratification
A personal history of cancer increases a patient’s risk for recurrence or secondary malignancies. Studies show that cancer survivors may face a higher likelihood of developing new cancers compared to the general population, reinforcing the importance of ongoing screening and surveillance. This code helps identify patients who may benefit from:
- Earlier or more frequent screenings
- Tailored preventive care plans
- Long-term monitoring strategies
This makes the code especially relevant in primary care and preventive medicine settings.
Public Health and Population-Level Significance
Beyond individual patient care, Z85.9 contributes to:
- Cancer survivorship research
- Population health analytics
- Healthcare planning and policy development
Accurate reporting allows public health agencies to better understand survivorship trends, allocate resources, and plan long-term care strategies for an expanding survivor population.
Conclusion
At Healthsure Hub, we emphasize the importance of accurately documenting a patient’s cancer history using ICD-10-CM code Z85.9. This code indicates a past malignant neoplasm that is no longer active and should be used only when the cancer site is unspecified. Proper use of this code not only supports billing accuracy and clinical decision-making but also reduces compliance risks and ensures high-quality, comprehensive patient records.