Head injuries are frequently evaluated in emergency departments, urgent care centers, and trauma settings. In some cases, the injury does not fit into a more specific ICD-10 category but is still clearly documented by the provider. Accurate code selection is essential for supporting medical necessity, maintaining coding compliance, and facilitating proper reimbursement.
Understanding when ICD-10 code S09.8XXA should be reported can help providers, coders, and billers accurately document head injuries during the initial stages of treatment.
What Does ICD-10 Code S09.8XXA Mean?
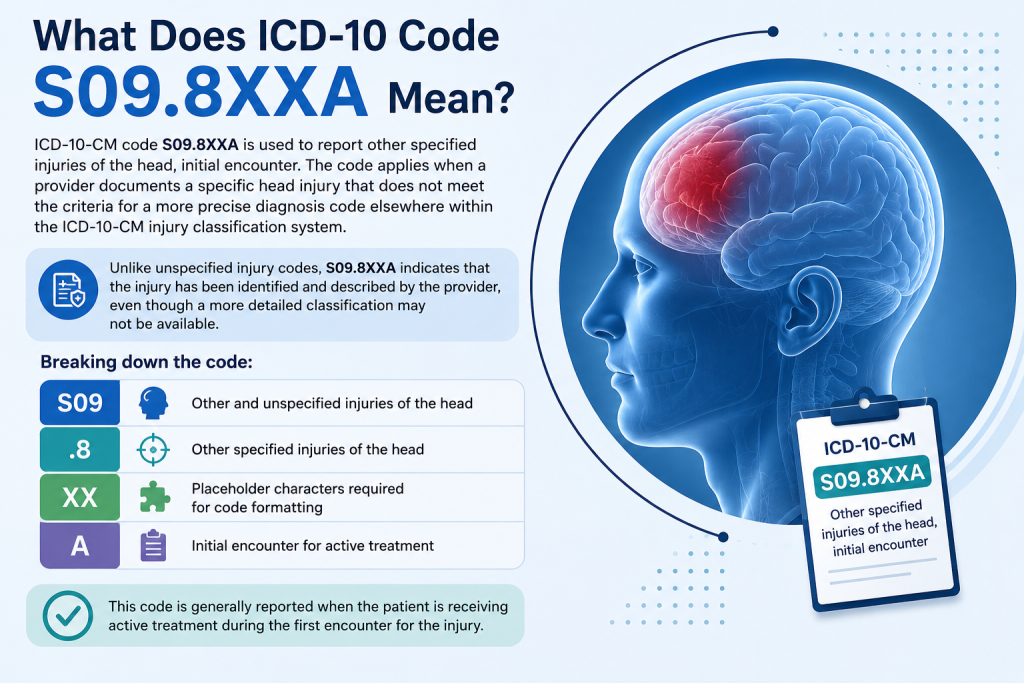
ICD-10-CM code S09.8XXA is used to report other specified injuries of the head, initial encounter. The code applies when a provider documents a specific head injury that does not meet the criteria for a more precise diagnosis code elsewhere within the ICD-10-CM injury classification system. Unlike unspecified injury codes, S09.8XXA indicates that the injury has been identified and described by the provider, even though a more detailed classification may not be available. Breaking down the code:
- S09 – Other and unspecified injuries of the head
- .8 – Other specified injuries of the head
- XX – Placeholder characters required for code formatting
- A – Initial encounter for active treatment
This code is generally reported when the patient is receiving active treatment during the first encounter for the injury.
When Is S09.8XXA Used?
S09.8XXA is used when documentation supports a specified head injury that is not classified elsewhere within the ICD-10-CM injury chapter.
Initial Trauma Evaluations
The code is frequently reported during the initial assessment of head injuries in emergency departments, urgent care clinics, and other acute care settings where active treatment is being provided.
Occupational and Accident-Related Injuries
Providers may assign S09.8XXA when evaluating head injuries resulting from workplace incidents, falls, motor vehicle accidents, or other traumatic events that require medical attention.
Cases Requiring Additional Evaluation
In some situations, diagnostic testing and clinical assessment may be necessary to fully characterize the injury. The code can be used when documentation supports a specified head injury but does not support a more precise ICD-10-CM classification.
Coders should always review available documentation to ensure a more specific diagnosis code is not supported by the medical record.
Documentation Requirements
Accurate documentation is essential when reporting S09.8XXA because the code falls within the “other specified” injury category. Unlike unspecified diagnosis codes, this designation requires providers to document enough detail to demonstrate the nature of the injury while supporting the selected diagnosis. Key documentation elements include:
| Documentation Element | Why It Matters |
| Description of the injury | Supports the use of an “other specified” injury code rather than an unspecified diagnosis. |
| Mechanism of injury | Provides clinical context and may support medical necessity. |
| Clinical findings | Documents the provider’s assessment and injury severity. |
| Diagnostic testing | Supports the diagnostic workup and treatment decisions. |
| Treatment provided | Demonstrates active management of the condition. |
| Encounter type | Confirms that the seventh character “A” is appropriate for the claim. |
Because injury claims often undergo detailed review, incomplete documentation can create coding uncertainty and increase the likelihood of reimbursement delays. Ensuring that the medical record clearly supports the diagnosis can help strengthen claim accuracy and reduce administrative rework.
Medical Necessity Considerations
Medical necessity plays a significant role in the reimbursement process for injury-related claims. While S09.8XXA is a valid billable ICD-10-CM code, the diagnosis alone may not be enough to support payment for services rendered. Payers often review the medical record to determine whether the evaluation, diagnostic testing, and treatment provided were reasonable and necessary based on the patient’s condition.
For this reason, documentation should clearly explain the circumstances surrounding the injury, the patient’s presenting symptoms, the provider’s clinical assessment, and any diagnostic studies ordered during the encounter. The record should also demonstrate how the findings influenced medical decision-making and treatment planning.
When documentation establishes a clear connection between the injury, the services performed, and the provider’s clinical judgment, it can help support medical necessity and reduce the claim denial rates or requests for additional information.
Billing and Coding Considerations for S09.8XXA
Accurate code selection is important when reporting S09.8XXA because multiple head injury codes may appear similar. Coders should review provider documentation carefully to ensure the selected diagnosis best reflects the documented condition.
Confirm the Injury Is Specifically Documented
Because S09.8XXA represents an “other specified” injury category, the medical record should clearly identify the injury being treated. Vague documentation may not support accurate code assignment.
Verify Encounter Designation
The seventh character “A” indicates active treatment during the initial encounter. Coders should confirm that the encounter type matches the documentation before claim submission.
Review for More Specific Codes
Before assigning S09.8XXA, coders should verify that a more specific head injury code is not available based on the documented diagnosis.
Accurate coding practices can help reduce reimbursement delays and improve claim accuracy.
Related ICD-10 Codes
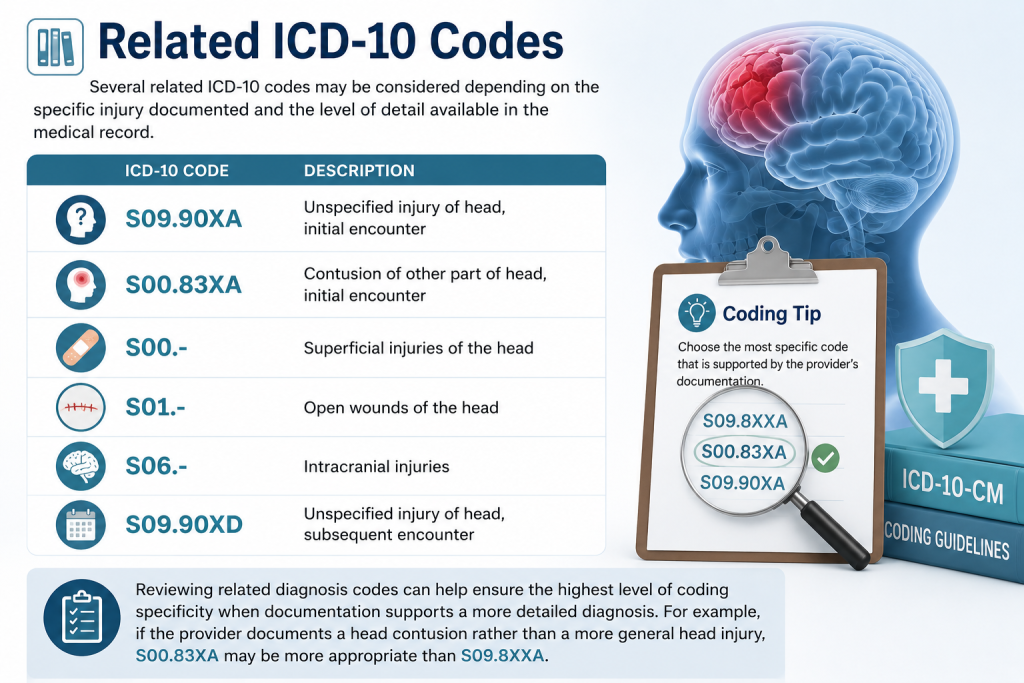
Several related ICD-10 codes may be considered depending on the specific injury documented and the level of detail available in the medical record.
- S09.90XA – Unspecified injury of head, initial encounter
- S00.83XA – Contusion of other part of head, initial encounter
- S00.- – Superficial injuries of the head
- S01.- – Open wounds of the head
- S06.– – Intracranial injuries
- S09.90XD – Unspecified injury of head, subsequent encounter
Reviewing related diagnosis codes can help ensure the highest level of coding specificity when documentation supports a more detailed diagnosis. For example, if the provider documents a head contusion rather than a more general head injury, S00.83XA may be more appropriate than S09.8XXA.
Final Thoughts
ICD-10 code S09.8XXA is used to report other specified injuries of the head during an initial encounter when the documented injury does not fit a more specific ICD-10-CM classification. Because the code represents a specified injury category, providers should ensure that the medical record clearly describes the nature of the injury and supports the diagnosis reported on the claim.
Accurate documentation, appropriate code selection, and ongoing review of clinical findings are essential for maintaining coding compliance and supporting reimbursement. When additional diagnostic information becomes available, coders should determine whether a more specific diagnosis code is warranted to ensure the highest level of coding accuracy.